
Turning the switch on? Ethical Issues of Deep Brain Stimulation for Psychiatric Disorders
Written by Y. Pooja Chowdary, Katuri Medical College
During the 1950s, the first experimental neuromodulation via brain electrodes was performed in patients with psychiatric disorders (Heath, Russell, Monroe, mickle, 1955). Since then, more than 120,000 neurological patients have been treated with Deep Brain Stimulation,1 whereas an estimated of only 500 psychiatric patients received DBS treatment (Benabid,2003; Naesstrom, Blomstedt, & Bodlund,2016). Why is that?
The answer lies back in the 1900s. With the ambivalent history of psychosurgery in mind, it is utterly comprehensible that even a reversible though (minimally) invasive technique like DBS invokes ancient fears. For instance, “The lobotomies performed by Moniz and freeman or the Tulane electric stimulation program by heath”.2
Popular fiction works, such as One Flew over the cuckoos Nest or The Manchurian Candidate, in which brain interventions are used to manipulate or abuse people, cross one’s mind.
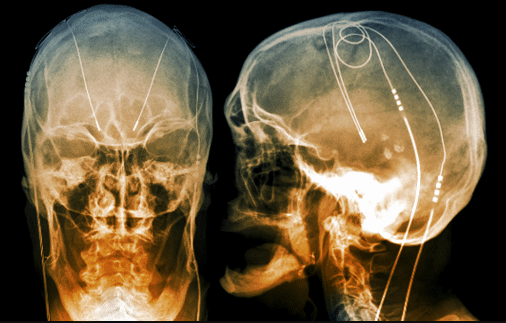
Unlike its precursor ablative procedures, Deep Brain Stimulation is a neurosurgical procedure in which electrodes are implanted into specific deep brain structures (thalamic & cerebellar nuclei) through the MRI guided stereotactical technique, and constant electric currents are applied via a neuromodulator (“brain pacemaker”) implanted in the chest. DBS has the benefit of being reversible, minimal lesion, and titratable to a patient’s symptoms. DBS has improved and intervention is much safer and creates minimal lesions.
Deep Brain Stimulation is a promising approach to the treatment of psychotherapy and pharmacotherapy-resistant psychiatric patients.
DBS was approved for the treatment of the refractory obsessive-compulsive disorder (OCD) in 2009 under a Humanitarian device exemption (HDE) by the FDA. Its application has been extended to treatment-resistant other psychiatric problems such as depression (rabies et al., 2009) and addiction.
Nevertheless, the costs of DBS are quite high over $50,000 per treatment and are covered by most insurance companies and Medicare only for FDA-approved targets. Off-Label uses are not covered, at least for now.3 The duration of the battery limits the choice of stimulation parameters, raises the treatment costs, and increases the risk of infection until improved devices with great longevity are developed.
While the cost of DBS is high, the social toll exacted by OCD and depression may well make this the treatment of choice for severe refractory patients should prove efficacious.
What are the key ethical issues of this? So because the patients have a refractor psychiatric illness will they make their own decisions or someone will make it for them? Who decides who gets the device? Will psychiatric patients be able to consent?
Patient selection should be conducted carefully, only severely afflicted and the treatment-refractory patient should be included and voluntary informed consent should be obtained.
“In the 1950s, Dr. Robert Heath, Tulane University conducted psychosurgery primness on the decapitated black inmate prisoners without consent”.
So Regardless, of past abuses to psychosurgery, informed consent of the individuals must be scrupulously safeguarded, with stringent and transparent patient selection. Authentic Informed consent can be challenging in psychiatric patients because issues include concerns about the competence of persons with severe mental illness toggle authentic informed consent. Some patients may be desperate because of their hopeless situation6 and they may feel that they have no other option but to consent to the proposed treatment but it doesn’t imply that the consent isn’t voluntary.
So from a legal perspective, can the court order DBS for social control (in the case of criminals and prisoners) against their will? This is when informed consent must stay intact. DBS can be performed only when the psychiatric patient consents voluntarily (Synofzik and Schlaepfer,2008).
Moreover, the acute, rapid changes that DBS can bring about, can disrupt the normal, “narrative flow of life” (Schechtman, 2010) and it may take time and effort for the patient to pick up and continue their life story.
The principal ethical concerns raised by DBS are: Are there any significant personality changes or not? If there is a personality change does this change say who they are or dehumanize them by altering their nature?
In DBS used for a psychiatric disorder, the stimulation specifically targets cognition, mood, and behavior; elements that are closely linked to the patient’s personality. There is a potential to cage – reversibly and reproducibly – individuals’ personalities. Social concerns arise, when these changes in personality and behavior negatively affect others, this may raise the problem of responsibility (Schermer, 2009b).
“If someone acts in a morally or legally bad way, can we hold this individual responsible when it is claimed that the accused personality is not the personality who acted?” 4
Although the long-term effects of DBS in psychiatric patients are still under investigation. DBS can be turned off immediately if side effects occur. DBS offers the opportunity to continuously adjust stimulation variables for each patient to optimize therapy.5 But the issue is the patient’s control over the devices. Due to their psychiatric condition, should these patients be constricted in their free decision-making process.?
If treatment is indeed easily inducible by “simply turning the switch on”, there is a danger of misuse of DBS, for mind control or over-enhancement of normal (healthy) cognitive function (“brain doping”; Fuchs, 2006; Ford, 2007). Priority should be set for “seriousness of impairment” over “chance to benefit ”.
The media often shapes public attributes about the use and funding of the latest neurotechnology devices. Investigators working with DBS should work with the media to ensure that accurate information is provided to policymakers and the public.
It would be unethical to abandon a possible beneficial treatment only for historical reasons.
To develop DBS to the level of standard therapy for psychiatric disorders, we need answers to “Who has the right to control mental condition ?” And “Who makes the decisions“ on “How much control is appropriate?” in daily life.
With all this in mind should the switch be turned on?
REFERENCES
- Graat, I., Figee, M. and Denys, D., 2017. The application of deep brain stimulation in the treatment of psychiatric disorders. International Review of Psychiatry, 29(2), pp.178-190.
- Schermer, M., 2011. Ethical issues in deep brain stimulation. Frontiers in Integrative Neuroscience, 5.
- Leaps. 2018. Deep Brain Stimulation for Mental Illnesses Raises Ethical Concerns.
- Klaming, L. and Haselager, P., 2010. Did My Brain Implant Make Me Do It? Questions Raised by DBS Regarding Psychological Continuity, Responsibility for Action and Mental Competence. Neuroethics, 6(3), pp.527-539.
- Schläpfer, T. and Bewernick, B. (no date) “Deep brain stimulation: Methods, indications, locations, and efficacy”, Electroconvulsive and Neuromodulation Therapies, pp. 556-572. doi: 10.1017/cbo9780511576393.038.
- The development of deep brain stimulation for neurological and psychiatric disorders: clinical, societal and ethical issues. (2021). Available at: https://www.frontiersin.org/research-topics/127/the-development-of-deep-brain-stimulation-for-neurological-and-psychiatric-disorders-clinical-societ (Accessed: 11 April 2021).


